Our previous blog, Is healthcare in Wales really that different?, sets out some of the key features of the Welsh health and social care system, and key differences from other parts of the UK. Like other developed healthcare systems, the structure of the NHS in Wales has developed and evolved in response to population needs and political pressures, to create a complex and multi-layered system. To better understand how the system is governed and the incentives that drive behaviour, we set out to map the organisations supporting core functions and the flows of accountability and funds. This blog provides a brief overview of the structure of the system, as well as our reflections on the challenges of trying to develop this system map.
Previous work identifying priorities and challenges for health and social care in Wales highlighted the governance structures and incentives driving behaviours in the system as a poignant concern. This exercise represents a starting point in understanding how decisions are made within the system and WCPP is currently engaging with those from the sector to plan our next steps for work in this area.
Click to view in more detail
How is the NHS in Wales structured?
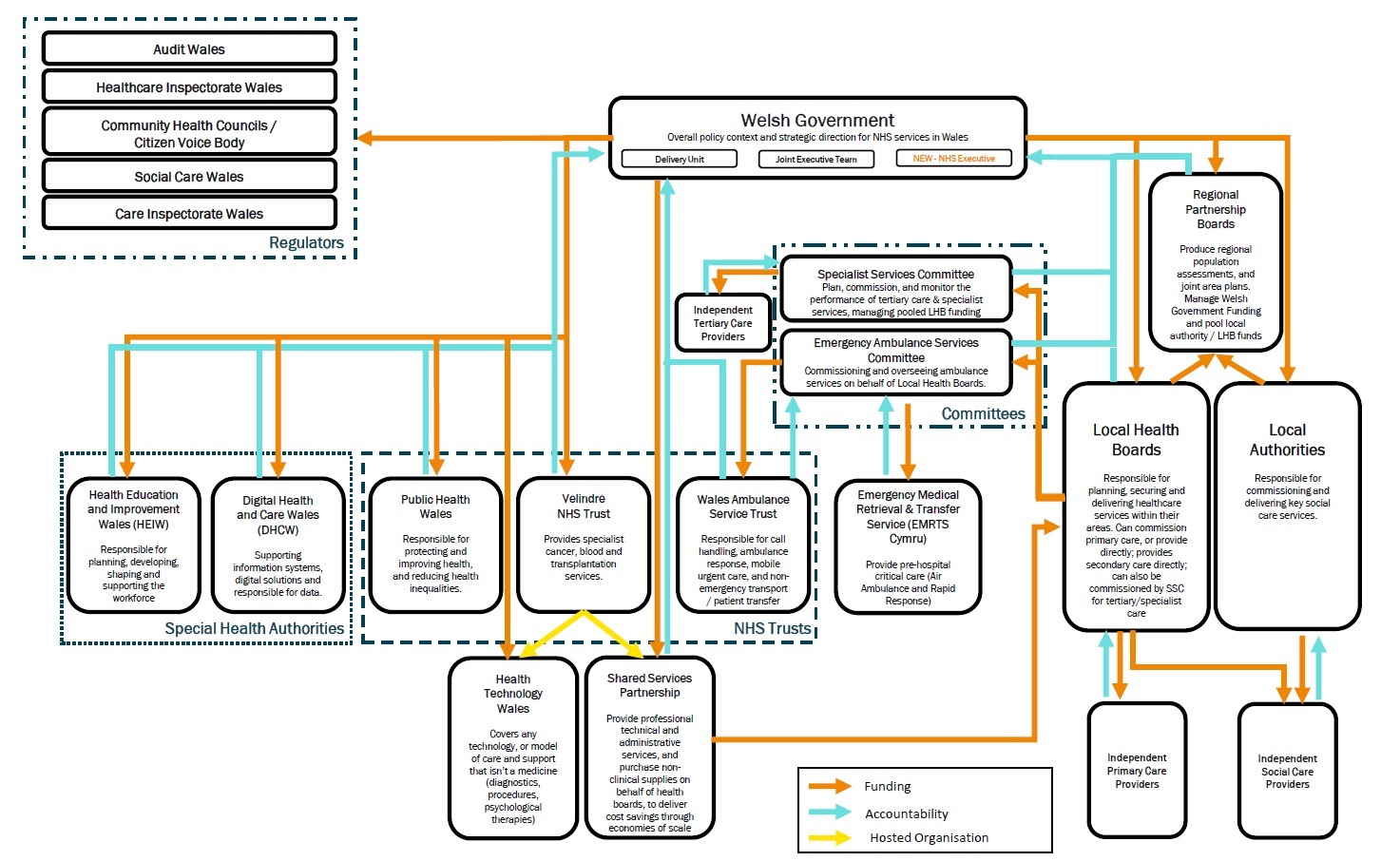
The multitude of organisations and the evolving nature of the system make it difficult to produce a definitive system map. However, broadly speaking, the system is formed of three tiers of organisations, with the first being formed of Welsh Government and the relevant regulators. Below that sit a variety of different bodies at both an all-Wales and regional level: these include local authorities, Local Health Boards (LHBs), the three all-Wales NHS Trusts and their hosted organisations, plus the two special health authorities. The Local Health Boards are responsible for a wide range of services, including hospital-based and community care for the population within their boundaries. They also commission a variety of primary care providers, including GPs, dentists, opticians, and pharmacists, who form the third level alongside the social care providers commissioned by local authorities and/or local health boards. Funding for Local Health Boards is via a specific core funding allocation from Welsh Government, based largely on the size and composition of the local population.
The three NHS Trusts and two special health authorities sit at roughly the same level as LHBs, but have an all-Wales remit. The NHS Trusts are largely responsible for providing public health, ambulance and cancer care services across Wales, while the special health authorities support the rest of the healthcare system in relation to both workforce planning (HEIW) as well as data and technology (DHCW). Like the Local Health Boards, they are accountable to Welsh Government, and produce Integrated Medium Term Plans to indicate how services will be commissioned and provided to meet the needs of, and improve outcomes for, the populations they serve. These plans usually cover a three year period, but have recently been more flexible in response to the global pandemic.
Healthcare services are regulated and inspected by Healthcare Inspectorate Wales, who also form one third of the tripartite escalation and intervention arrangements, alongside Audit Wales, the external organisation responsible for auditing NHS bodies, and Welsh Government, who manage the day-to-day performance of the NHS through a variety of performance indicators. This is one example of the strong and centralised role played by Welsh Government within the system. Welsh Government also centralise responsibility relating to strategy and priorities as well as the distribution of resources. Moreover, the recent announcement of the NHS Executive as a senior team sitting within Welsh Government, rather than a standalone body, reaffirms a commitment to this centralised way of working. Our blog on the formation of the NHS Executive discusses this in more detail.
Challenges of mapping the system
Mapping the system proved a challenging exercise for two main reasons. Firstly, there is simply a multitude of different organisations of varying sizes, and there are too simply many to name and situate within the general structures that underly the system. A notable example of this is the various teams and committees represented within Welsh Government, including the Delivery Unit and Joint Executive Team, amongst others. Each of these takes on its own responsibilities and accountabilities within the system, and it is unclear how much coordination there is between them. This is also where the new NHS Executive will sit within the health and social care system, further convoluting matters.
Secondly, organisations within the system emerged and have since evolved in their own way over time, making it difficult to categorise and group the ever-moving parts. For example, Wales has three NHS Trusts that deliver services across the nation: the Welsh Ambulance Service Trust, Velindre NHS Trust, and Public Health Wales. Yet, while all three organisations are badged as NHS Trusts, they all have different structures of funding and accountability that are determined by their respective functions and origins. The two Special Health Authorities (Health Education and Improvement Wales and Digital Health and Care Wales) also have an all-Wales remit, but evolved differently and more recently, and take on an altogether different function.